AUCTORES
Globalize your Research

Case Report | DOI: https://doi.org/10.31579/2578-8949/018
*Corresponding Author: Swathi Goli, Department of Pharmaceutics, Vikas College of Pharmacy, Warangal, India.
Citation: Swathi Goli and Prasad Garrepally, Pressure Ulcers in Spinal Cord Injury Patients Frequently Require a Dedicated Reconstructive Plastic Surgeon. J .Dermatology and Dermatitis. Doi: 10.31579/2578-8949/018
Copyright: © 2018 Swathi Goli. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Received: 04 January 2018 | Accepted: 24 January 2018 | Published: 29 January 2018
Keywords: pressure ulcers; unrelieved pressure; tissue shearing
Pressure ulcer formation is the result of unrelieved pressure, tissue shearing, and localized ischemia over a bony prominence resulting in cell death and tissue necrosis. The incidence of pressure ulcers in the spinal cord injury population is estimated between 25 – 66%. When meticulous wound care, control of infection, local debridement, and pressure offloading fail, patients require wound excision and vascularized soft tissue reconstruction. Recurrence rates of chronic ulcers are high, reported over 30%, ultimately resulting in multiple operations and eventual exhaustion of all other local tissue flaps. Lower extremity disarticulation and total thigh flap is the last resort treatment for the reconstructive surgeon. This report describes a paraplegic patient with T6 complete spinal cord injury with recurrent sacrococcygeal and bilateral ischioperineal pressure ulcers requiring right lower extremity disarticulation and total thigh flap.
Pressure ulcers are skin and soft tissue wounds caused by unrelieved pressure resulting in irreversible cellular necrosis. These lesions develop secondary to local ischemia caused by blood vessel occlusion from longstanding pressure combined with the sheer force of soft tissue movement against bony prominences [1]. Moisture is a major contributing factor in the development of pressure ulcers because any excess fluid resulting from incontinence, excessive sweating, excessive vaginal discharge, or wound discharge can cause maceration of the epidermis and increase susceptibility to ulcer formation [2].
Many groups of patients are at high risk of developing pressure ulcers including immobile, bedridden and insensate patients, especially those with spinal cord injury (SCI) who have an annual incidence rate between 20 and 31 percent [3]. The 3 major risk factors for the formation of pressure ulcers in SCI patients are loss of sensory perception, loss of motor function and moisture from bowel and bladder incontinence. SCI patients do not sense pain when their tissue becomes ischemic from long-standing pressure and do not move their body to relieve pressure. Additionally, they lose the alpha adrenergic nerve fibers that control vascular tone, which increases the likelihood of vascular occlusion [1].
The most common sites of pressure ulcer formation are the sacral and ischial prominences, but pressure ulcers also commonly develop at the femoral greater trochanter, elbow, heel, scapula, iliac crest, and malleolar regions [1]. The location of formation varies depending on the patient’s typical positions while immobilized. The treatment for pressure ulcers ranges from medical to surgical depending on the severity, complications, and comorbidities. Medical treatment consists of thorough debridement of necrotic tissue, pressure offloading, nutritional optimization, control of infection, removal of soiling bodily fluids, and meticulous wound care. When medical treatments fail to heal the chronic pressure ulcer, surgical treatment should be considered. The mainstay of surgical treatment is complete wound excision including debridement of colonized and osteomyelitic bone and vascularized soft tissue reconstruction. Here we present a case of recurrent sacrococcygeal and bilateral ischioperineal ulcers with a urethral fistula requiring left gluteus maximus flap readvancement and right lower extremity disarticulation with total thigh flap.

Clinical history
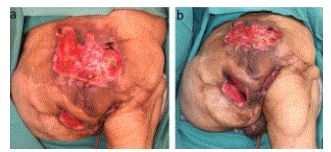
The patient is a 56 year old paraplegic male with T6 complete spinal cord injury secondary to gunshot wound 25 years prior and complex past medical history including Hepatitis C infection, deep vein thrombosis and pulmonary embolism with inferior vena cava filter placement, intravenous drug abuse currently on methadone, achalasia requiring Botox (Allergan, Dublin, Ireland) injection, and chronic anemia. His surgical history included partial colon resection with colostomy and Hartmann’s pouch, urinary bladder augmentation, multiple debridements, bilateral gluteus maximus advancement flaps, bilateral gracilis flaps, bilateral girdlestone procedures with vastus lateralis flaps, and left leg disarticulation with total thigh myocutaneous flap closure of bilateral ischial pressure ulcers. Following recurrence of his pressure ulcers, an outside hospital initially treated this ulcer through debridement but removed his suprapubic bladder catheter resulting in urine leakage into the open wounds and further contributing to wound necrosis. He presented to our clinic 1 year after his left leg disarticulation and total thigh flap with an extensive stage IV sacrococcygeal pressure ulcer and bilateral stage IV ischioperineal pressure ulcers with erosion into the perineal urethra. The right stage IV ischioperineal ulcer measured 9cm x 5cm x 6cm with 8cm medial undermining beneath bridging perineal tissue. The left stage IV ischioperineal ulcer measured 10cm x 6cm x 5cm with 8cm medial undermining in continuity with the right ischioperineal wound. The two ischial ulcers communicated and fistulized into the exposed perineal urethra. The wounds were clean with notable urine leakage into the ulcers and pink granulation tissue without evidence of active infection. The stage IV sacrococcygeal ulcer measured 12.5cm x 17cm x 2.5cm and the wound appeared clean with areas of necrotic tissue and pink granulation tissue without evidence of active infection (Figure 1).
Prior to surgery, central venous access was established through a right internal jugular tunneled central venous catheter. Urinary diversion was performed through open cystostomy with suprapubic bladder catheter placement. The patient also had a urethral catheter which spanned the ulcer through the perineal urethra and entered the bladder neck.
The patient was positioned in the prone position after padding all bony prominences using Allevyn adhesive foam (Smith & Nephew, London, UK).
The sacrococcygeal ulcer was first excised down to the level of the sacrum using electrocautery. The skin bridge separating the sacral ulcer from the more inferior ischioperineal wounds was excised taking care to avoid the anus. The wound was excised in its entirety throughout the bilateral ischioperineal wounds Operative procedure(Figure 2). There was significant heterotopic ossification at the area of the left hip which was excised. The wounds were thoroughly lavaged using 3L of normal saline mixed with 50,000 units of bacitracin.
The patient’s Foley catheter was used to localize the penile urethra, bladder neck and ulcerated perineal urethra Operative procedure(Figure 2). The Foley catheter was removed and the bladder neck was ligated using 2-0 Vicryl suture (Ethicon, Cincinnati, OH) Operative procedure(Figure 3). A segment of pelvic floor including the perineal body was mobilized by electrocautery using a random flap design and turned over in order to provide soft tissue reinforced closure of the bladder neck. The penile urethra was then closed using a running 2-0 Vicryl suture and then oversewn using an additional layer of interrupted sutures. The skin bridge between the ischioperineal wound was converted into an inferiorly based random flap, de-epithelialized and used to reinforce soft tissue coverage of the penile urethra.
The previously performed left gluteus maximus flap was reincised along the lateral, superior, and medial scar edges and elevated down to the level of the gluteus maximus muscle. The flap was incised through the investing fascia of the gluteus maximus to allow for mobilization. A Burow’s triangle back-cut was performed along the inferior border of the flapto provide increased mobilization without separating the inferior skin paddle. The gluteal flap was re-rotated toward the midline for closure of the left half of the sacral wound.
The sacrococcygeal and right ischioperineal wounds were reconstructed using right lower extremity disarticulation and the total thigh flap (Figure 4). A previous longitudinal incision along the lateral aspect of the right thigh, made during the prior Girdlestone and vastus lateralis flap procedures, was re-incised and extended along the lateral aspect of the leg from the hip down to the knee. Scar tissue was incised down to the lateral aspect of the upper third of the femur. The tissues of the posterior, medial, and anterior thigh were dissected from the femur using electrocautery and taking care to avoid the profunda femoris vascular bundle. The popliteal artery and vein were ligated using 3-0 Vicryl suture ligatures. A circumferential incision was made at the femoral condyles to separate the femur entirely from the total thigh flap. Hemostasis was achieved throughout the total thigh flap operative field using electrocautery as well as suture ligatures. The femur and lower leg was submitted to pathology for examination.
One Shirley sump drain was placed in the ischioperineal wound exiting through the right lateral buttock. A second sump drain was placed in the sacrococcygeal wound exiting the left lateral buttock. Thrombin soaked Avitene (Davol, Warwick, RI) collagen sponge was applied over the sacrum, ischium and wound bed for hemostasis. The deep layers of the flap were closed first approximating fascia when possible using a series of interrupted 0 Vicryl. The deep dermis and skin were closed using Vicryl, Monocryl, and Prolene (Ethicon, Cincinnati, OH) (Figure 5). Following complete closure, the wounds were then dressed in Bactroban (GSK, Brentford, UK), Xeroform (DeRoyal, Powell, TN), gauze, and abdominal pads that were silk taped in place.


Pressure ulcers are staged based on their clinical appearance and involvement of the underlying soft tissue. Stage I ulcers represent an acute inflammatory response marked by non blanchable erythema, induration, warmth, and firming of the skin. Stage II ulcers appear as a blister or abrasion and involve the epidermis and possibly part of the dermis. Stage III ulcers are defined by extension of the lesion into the soft tissue without involvement of the underlying muscle. Stage IV ulcers extend into the underlying muscle, bone, or joint space with the possibility of undermining or sinus tract formation [4]. Staging of pressure ulcers is important for guiding treatment and determining prognosis.
Surgical reconstruction of pressure ulcers is indicated when wounds do not heal despite medical management including debridement of necrotic tissue, pressure offloading, meticulous wound care, control of infection and body fluid contaminants, and optimal nutrition. Other indications for surgery include progression in the size of the ulcer, extension of the ulcer into tissue or bone causing osteomyelitis or sepsis, development of ulcers in insensate areas causing extensive necrosis with bacterial colonization, extension of the ulcer into vital organs such as the hip joint, urethra or vagina, development in a newly injured spinal cord injury patient, or quality life interruption [1]. There are many important factors to consider when determining the appropriate surgical technique including the patient’s primary disease that contributed to ulcer formation, possible impairment of motor function, first-time or recurrent ulcer, and prior surgical reconstructions performed [1].
Lower extremity disarticulation and total thigh flap is an operation that is used only as a last resort when other reconstructive options have been exhausted, but can be life-saving for patients who are severely disabled and otherwise face progression of the wound, further damage to vital organs, infection, sepsis, and death [1]. Leg disarticulation and total thigh flap is considered when the patient has failed multiple local flap reconstructions and no other myofascial, myocutaneous, no rfasciocutaneous flaps are available to use for wound closure. In the past, leg disarticulation with total thigh flap was typically performed as a two-step procedure, first debriding and amputating the leg, and secondarily in-setting the total thigh flap for closure of the wound. However, in 1992 it was found that in setting the flap during the second procedure was complicated by formation of early heterotopic ossification within the muscles during the time interval between procedures [5].The single-stage operation is now preferred where in the wound is prepared, the leg amputated and the total thigh flap inset during a single operation.
Pressure ulcer reconstruction is complicated by high rates of postoperative complications ranging from 6.6-53% [6]. There are many factors that increase the risk of complications such as chronic infection, vascular necrosis of skin and deep tissue, urine or fecal contamination, muscle spasms in the perioperative period, poor patient compliance, and excessive blood loss during the operation and anemia. Complications specific to soft tissue reconstruction procedures include seroma, hematoma, wound infection, fat necrosis, wound dehiscence, and flap necrosis, with seroma being the most common [1].

Pressure ulcers in spinal cord injury patients frequently require a dedicated reconstructive plastic surgeon capable of performing a variety of flap types for recurrent ulcers in addition to taking a multidisciplinary approach toward care. SCI patient’s insensitivity predisposes them to recurrence of wounds, particularly in the sacral and ischial areas, that are often complicated by infection or invasion into local organs. When all other reconstruction options are exhausted, lower extremity disarticulation with total thigh flap provides a last resort for wound closure.
Clearly Auctoresonline and particularly Psychology and Mental Health Care Journal is dedicated to improving health care services for individuals and populations. The editorial boards' ability to efficiently recognize and share the global importance of health literacy with a variety of stakeholders. Auctoresonline publishing platform can be used to facilitate of optimal client-based services and should be added to health care professionals' repertoire of evidence-based health care resources.



























































